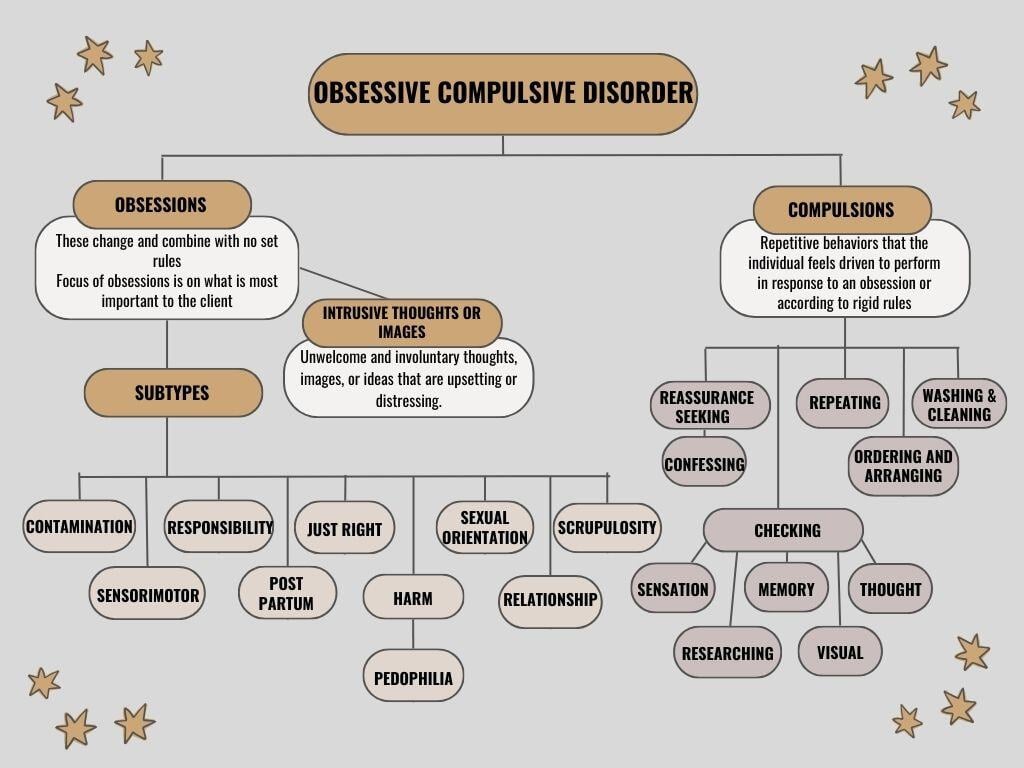
Obsessive-compulsive disorder (OCD) presents itself in nuanced, multifaceted ways. Subtypes of OCD can be conceptualized based on the nature of a client’s obsessions and compulsions (repetitive behaviors). Although every individual’s experience is shaped by their context, emotions, values, and stressors, exploring these subtypes can offer a deeper awareness of the patterns that sustain OCD’s grip on their lives.
Understanding these categories helps therapists design exposures for treatment. When I say exposures, I am referring to Exposure and Response Prevention (ERP) therapy, which is the gold standard treatment for obsessive-compulsive disorder (OCD). ERP works by gradually exposing individuals to their fears or triggers while abstaining from the compulsive behaviors. This method creates new learning to inhibit the old OCD learning ultimately creating freedom from OCD. Understanding these categories, is the first step in treating OCD.
Contamination and Cleaning OCD
This subtype reflects a search for purity or safety-a need to physically or psychologically disconnect from perceived danger.
- Obsessions: Intense fear of germs, dirt, or any form of contamination (e.g., touching doorknobs or public surfaces), or "dirty" or sinful people.
- Compulsions: Relentless cleaning, compulsive handwashing, or complete avoidance of perceived contaminants.
Therapist Tip: Shift the lens of focus from external germs to the internal distress they represent. Use Exposure and Response Prevention (ERP) to help clients tolerate the discomfort of not performing compulsions.
Checking OCD
Imagine living with the debilitating fear that one minor oversight could lead to catastrophe. For those with Checking OCD, this fear governs their daily life.
- Obsessions: Intrusive doubts and fears of causing harm, making mistakes, or setting off disastrous events (e.g., forgetting to turn off the stove, leaving doors unlocked).
- Compulsions: Endless checking of locks, appliances, or documents-fueled by an effort to neutralize imagined harm.
Therapist Tip: Reframe the relationship with uncertainty. Help clients recognize that it’s their intolerance of doubt-that perpetuates their checking cycles. Teaching our clients to tolerate the uncertainty of "danger" .
Just Right OCD
For these clients, feeling just right is necessary for inner peace.
- Obsessions: Profound discomfort when objects or occurrences feel asymmetrical, out of order, or "imperfect."
- Compulsions: Repeatedly arranging, ordering, or aligning objects, or redoing actions until they “feel right.”
Therapist Tip: Attune to the deeper emotional drivers. Explore how disordered external chaos may mirror clients’ discomfort with disorder within and use ERP to break perfectionistic cycles.
Silent suffering wrestles internally with taboo or distressing thoughts.
- Obsessions: Recurrent, graphic, and unwanted thoughts (e.g., violence, sex, moral transgressions, or blasphemy).
- Compulsions: Covert mental rituals-such as reassurance-seeking, rumination, or analyzing their own thoughts for "proof" of safety.
Therapist Tip: Normalize thought content without assigning danger to its presence. Use ACT (Acceptance and Commitment Therapy) alongside ERP to teach clients to accept, rather than fight, the fleeting nature of unwanted thoughts.
Harm OCD
For clients with Harm OCD, even benign objects or situations are transformed into overwhelming threats.
- Obsessions: Fear of unintentionally harming oneself or others (e.g., stabbing someone, pushing pedestrians, being a serial killer, killing someone in their sleep).
- Compulsions: Avoidance of specific situations, seeking reassurance from others, avoiding tools or knives scissors, or repetitive checking to ensure harm has not occurred.
Therapist Tip: Unpack avoidance behaviors. Gradually expose clients to tools, and build an acceptance of intrusive thoughts without yielding to safety behaviors (compulsive behaviors).
Relationship OCD (ROCD)
ROCD takes the vulnerability of love and attachment and twists it into relentless questioning and doubts.
- Obsessions: Intrusive fears about the viability of relationships (e.g., "Am I really in love?" "What if they're not 'the one'?").
- Compulsions: Comparing relationships, seeking reassurance from others, or analyzing compatibility endlessly.
Therapist Tip: Guide clients away from resolution-seeking, reinforcing the idea that certainty in relationships is neither attainable nor necessary for healthy love.
Sexual OCD
For individuals with Sexual OCD, intrusive sexual thoughts do not reflect attraction or desire but evoke deep discomfort and fear.
- Obsessions: Troubling thoughts about inappropriate sexual behaviors or attractions (e.g., fears of incestuous attraction or sexual violence).
- Compulsions: Avoiding potential triggers, seeking reassurance, or mentally evaluating arousal.
Therapist Tip: Defuse the stigma around intrusive thoughts. Foster an environment free of shame where clients can openly discuss fears and engage in ERP to confront, rather than evade, their triggers.
Pedophilia OCD
This involves intrusive, unwanted thoughts or fears about inappropriate sexual behavior, which can cause significant distress.
- Obsessions : Individuals may experience persistent, intrusive thoughts or images involving fears of harming or acting inappropriately with children, despite having no desire or intent to do so.
- Compulsions: To reduce anxiety, individuals may engage in repetitive behaviors such as seeking reassurance, avoiding triggers, or mentally reviewing past interactions to ensure no inappropriate behavior occurred.
Therapist’s tip: Gradually exposing your client to their triggers while teaching them to refrain from compulsive behaviors, helping to reduce their power over time.
Religious or Scrupulosity OCD
Clients with this subtype take moral integrity or religious adherence to extreme, debilitating levels.
- Obsessions: Fear of being sinful, offending God, or not following religious rules to perfection.
- Compulsions: Excessive praying, seeking reassurance from religious figures, or confessing perceived wrongdoings.
Therapist Tip: Collaborate with spiritual leaders if appropriate, and help clients explore the difference between spiritual devotion and compulsive behaviors that stem from fear rather than faith.
Existential or Philosophical OCD
For some, the vastness of existential questions becomes a mental trap rather than a source of wonder.
- Obsessions: Overwhelming thoughts about life’s meaning, the reality of existence, or the nature of the universe.
- Compulsions: Unending rumination, searching for philosophical answers, or questioning one’s perceptions of reality.
Therapist Tip: Redirect clients to the present moment through mindfulness techniques while teaching them that some questions are meant to coexist with curiosity, not certainty.
Somatic or Sensorimotor OCD
This subtype traps clients in an endless loop of focusing on involuntary bodily processes.
- Obsessions: Heightened awareness of natural body sensations (e.g., breathing, heartbeats, blinking) or specific physical conditions.
- Compulsions: Efforts to monitor, control, or mentally evaluate these sensations.
Therapist Tip: Interrupt hyperawareness cycles with refocus exercises that ground clients in external stimuli rather than internal sensations.
False Event OCD
A subtype of OCD where individuals become obsessed with the fear that they have caused or been involved in an event that never actually happened.
- Obsessions: Intrusive thoughts or doubts about committing a bad act, such as lying, cheating, harming someone, or causing an accident. Fixation on incomplete memories, interpreting them as evidence of wrongdoing. Intense guilt, shame, or fear over a possible past action.
- Compulsions - This can lead to intense doubt, guilt, and repeated attempts to seek reassurance or uncover "proof" of their innocence.
Therapist TIP: Focus on exposing clients to the uncertainty and discomfort of the intrusive thought without seeking reassurance or engaging in compulsions. This helps train your brain to tolerate uncertainty and reduces the power of the obsession over time.
Real Event OCD
involves obsessive thoughts and guilt over past actions or events. Individuals may fixate on whether they acted appropriately or morally in certain situations, often replaying the event in their minds and doubting themselves repeatedly.
- Obsessions: Individuals with Real Event OCD often become preoccupied with past actions or events, worrying excessively about their consequences or moral implications. These intrusive thoughts can cause significant distress and self-doubt.
- Compulsions: To cope with these obsessions, individuals may repeatedly analyze the event, seek reassurance from others, or mentally replay the situation in an attempt to find certainty or relief.
Therapist TIP: Focus on gradually exposing yourself to the thoughts or memories causing distress without engaging in compulsive behaviors. This helps you build tolerance to the anxiety and reduces the need to seek reassurance.
Retroactive OCD
This form of OCD involves persistent doubts or intrusive thoughts about past actions, decisions, or events, often leading to excessive rumination and a need for reassurance.
- Obsessions: Intrusive thoughts or doubts about past actions, decisions, or events, often leading to excessive rumination and questioning.
- Compulsions: Repeated mental or physical actions aimed at seeking reassurance, reviewing past events, or attempting to "undo" perceived mistakes.
Therapist TIP: Focus on gradual exposure to intrusive thoughts while resisting the urge to ruminate or seek reassurance. This approach helps reduce anxiety over time and builds resilience.
Postpartum OCD
A condition that can affect new parents, causing intrusive thoughts and compulsive behaviors related to the safety and well-being of their baby.
- Obsessions: Intrusive, unwanted thoughts that cause distress, often related to the baby’s safety or well-being.
- Compulsions: Repetitive behaviors or mental acts performed to reduce the anxiety caused by the obsessions, such as excessive checking or cleaning.
Therapist Tip: Gradually expose clients to triggering thoughts or situations while resisting the urge to perform compulsions.
Supporting Clients Through Complexity
OCD may wear different masks, but at its core, it capitalizes on clients values and core fears. For therapists, understanding these subtypes empowers you to empathize, strategize, and intervene with greater precision.
Remember, individuals with OCD often battle shame, confusion, and isolation due to the nature of their thoughts and behaviors. Your role is not only to teach them skills for managing symptoms but also to help them reclaim their lives from a condition that distorts their perception of reality.
Normalize, Normalize, Normalize-let's break the stigma around OCD, the 4th most common mental health condition affecting millions of people worldwide. It's important to understand how OCD works and to avoid unintentionally becoming part of their OCD loop. Sometimes, what we think is helping can actually reinforce their OCD. By educating ourselves, we can provide support and guide them towards real change through ERP.
Explore our OCD series for further insights!


 KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED