 KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
KD HOLMES, LPC, EMDR CERTIFIED, BTTI TRAINED
Understanding Harm OCD and Finding Your Way Back to Yourself
Some fears arrive like thunderstorms-loud, visible, and unmistakable. Others creep in quietly, like fog-unwelcome, disorienting, and hard to explain....

There is a particular kind of fear that doesn’t just scare you-it makes you question who you are.
If you’re here, you may be dealing with intrusive sexual thoughts involving children that feel deeply disturbing and completely out of alignment with your values. This is often referred to as POCD (Pedophilia OCD), a subtype of obsessive-compulsive disorder.
These thoughts are not desires. They are not intentions. They are intrusive, ego-dystonic fears that attach to what matters most.
The good news-though it may not feel like it right now-is that this is highly treatable. Exposure and Response Prevention (ERP), a specialized form of cognitive behavioral therapy (CBT), is considered the most effective treatment for POCD.
If this feels familiar, keep reading. Understanding what’s happening is often the first step toward relief.
POCD is a subtype of OCD characterized by intrusive, unwanted thoughts or images about harming children sexually. These thoughts feel unbearable precisely because they are so violently out of alignment with the person’s values, desires, and moral compass. Sexual intrusive thoughts are extremely distressing to the sufferer. They intrude upon an otherwise normal moment.
Imagine a mother who avoids changing her baby’s diaper, not because she doesn’t love her child, but because her mind flashes images she didn’t invite and cannot unsee. Her distress isn’t born from attraction-it’s born from terror. This is POCD.
ERP is a specialized form of cognitive behavioral therapy (CBT)
The stakes are high for clarity here.
POCD is about fear. Fear of being a pedophile. Fear of losing control. Fear of harming the very people you care for. Fear of harming one of our most vulnerable populations, children.
Pedophilic Disorder, by contrast, involves enduring sexual attraction to children, often paired with justifications or lack of remorse.
Many clients with POCD come to therapy convinced they have Pedophilic Disorder, but trying to persuade them otherwise is not beneficial and not the approach we use to treat POCD. However, having a therapist trained in OCD treatment is crucial to avoid misdiagnosis.
Confusing the two is not just clinically damaging-it’s ethically reckless. POCD sufferers are often overwhelmed with guilt, and the mere act of seeking help can feel like a confession to a crime they haven’t committed.
This is why accurate diagnosis matters. This is why we need therapists who understand the diagnosis.
Each compulsion is an attempt to feel "clean" again. But compulsions never offer true peace, you get a moment of relief until the image or thought returns. And then the process starts all over again. In chasing the compulsions, the fear grows stronger. That's how OCD works-the more compulsions one does, the more anxiety they have.
ERP is not a punishment. It's not retraumatization. It's an act of radical trust-in the client, and in the process. ERP is the choice to stop arguing with fear and instead sit beside it.
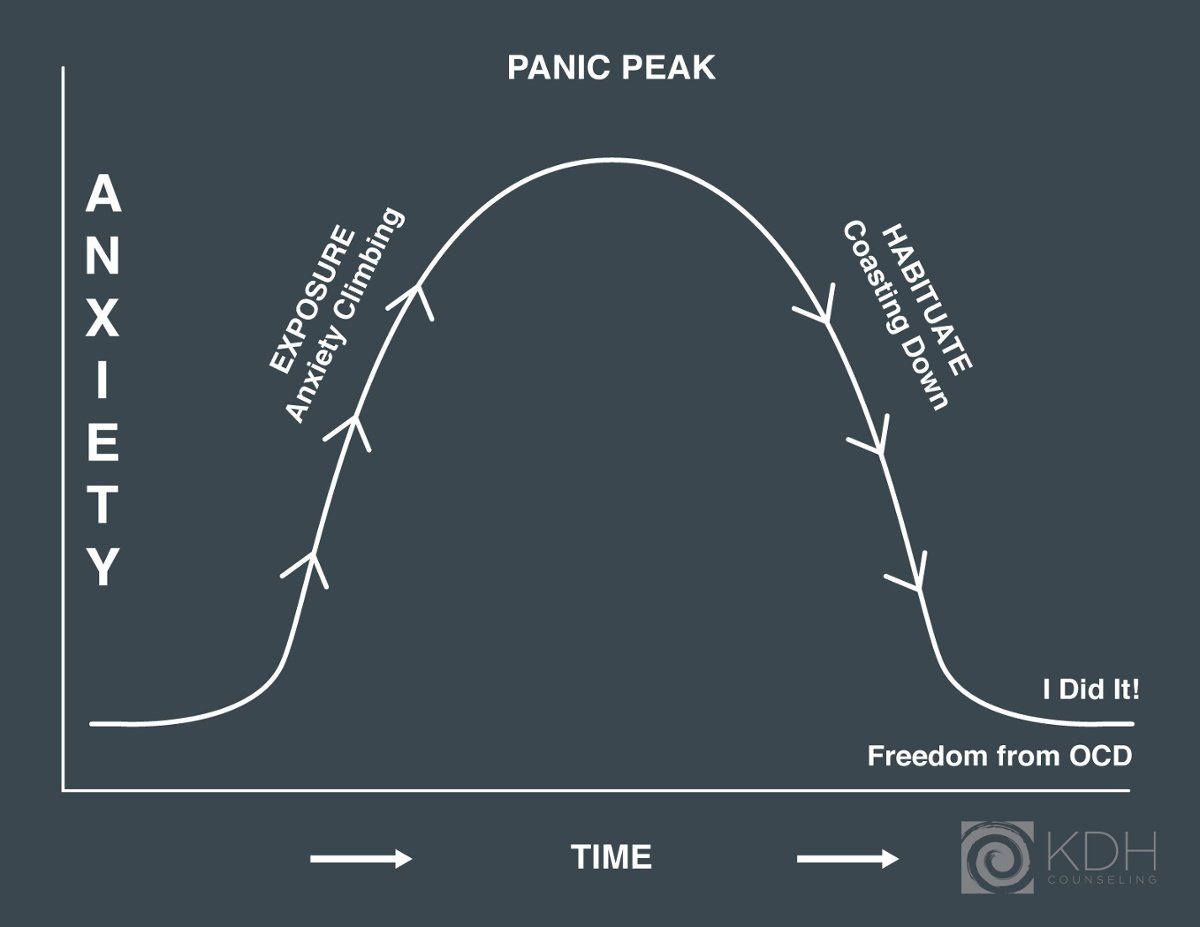
ERP asks us to face our worst fear. Courageously. It's not about proving the thoughts are untrue. If that worked, you would not be reading this blog. It's about learning these thoughts don't have to be answered. It's about learning we can coexist with these intrusive thoughts and images. And over time, we learn not to panic when they show up. They lose their edge.
In ERP, we are asking the brain to build tolerance to uncertainty and discomfort. This happens not through logic or reassurance, but through experience . We expose ourselves to the trigger and then-this is the hard part-we prevent the compulsive response. That means we do not check, do not ask, do not google, do not mentally replay. We sit with the fear.
This repetition is essential. Not once. Not a few times. But again and again until the client learns they can be with these thoughts and images. ERP works by helping our nervous system recalibrate. We teach our body, through lived experience, that distress is survivable-and that we are trustworthy in the face of it.
Looking at a picture of a child and allowing the thought to come-without scrambling to erase it.
Writing a detailed exposure script with a therapist and reading it out loud receptively until the words become gibberish.
Spending time with nieces or nephews without avoiding physical touch, and without dissecting the experience afterward for “proof” of wrongdoing (abstaining from compulsions).
ERP isn’t about acting on fear-it’s about sitting beside it again and again and again. Courage isn't the absence of anxiety; it's the refusal to let it make your choices.
Tanya was 21 when she came to therapy, eyes downcast, voice low. She wouldn’t go near the student center on campus because there was a preschool nearby. She believed avoidance made her and children safe.
In therapy, we built an ERP heirarchy. The first step: walking past the preschool without crossing the street. Then: watching videos of children playing. Eventually: volunteering at a childcare event-surrounded by kids, holding his ground, letting the thoughts come, and learning to face the OCDemon.
Tanya didn’t become fearless. She became free. She learned that thoughts are not prophecies, and that she could face and feel fear and terror without doing compulsive behaviors.
ERP is structured, safe, and never involves illegal behavior. Therapists ensure exposures are clinically sound and ethically appropriate. No one is ever asked to act out harmful behavior. Instead, they confront the fear of such behavior.
ERP isn’t a thought-deletion tool. It’s a practice of learning how to live with uncertainty. With time, the thoughts lose their grip. They come, and they go. And eventually, you know what to do with them.
While SSRIs can help, ERP alone is effective for many. The key is consistent, skilled delivery. ERP offers a 65–80% success rate when done properly. That’s not just data. That’s hope. But some people find symptoms decrease in intensity with medication.
Finding the right therapist when you're experiencing POCD is crucial-and not every well-meaning clinician is equipped to treat it effectively. Here's what to look for:
Training in ERP: Your therapist should have specific training in Exposure and Response Prevention. Ask directly. ERP is the gold standard for OCD, and POCD requires particular sensitivity and structure. BTTI training is the best training a therapist can receive.
Comfort with taboo thoughts: Your therapist must be someone who can sit with If you’re recognizing yourself in this, you are not alone—and you do not have to navigate it on your own. Working with a therapist trained in OCD and ERP can make a significant difference.
If you’re ready to explore treatment, our team provides evidence-based OCD therapy in Lafayette, Louisiana, with both in-person and telehealth options across the state.
You can schedule a consultation or learn more about working with an OCD specialist here.
the content of your fears without flinching, pathologizing, or rushing to reassure. This work requires a clinician who understands that intrusive thoughts are symptoms-not signals.
Experience with OCD: General anxiety experience is not the same as OCD expertise. POCD involves complex mental compulsions and fears of moral failure. You want someone who speaks that language fluently.
Nonjudgmental and grounded: The shame around POCD can be paralyzing. You’ll need a therapist who can model calmness, curiosity, and deep compassion-even as you share your most feared thoughts.
Avoids reassurance and talk therapy models: If your sessions keep veering into talking about why you have the thoughts or why they're unlikely to be true, you may not be doing ERP. Effective treatment involves facing the thoughts, not analyzing or defusing them endlessly.
You deserve treatment that honors your bravery and offers you a path forward. Keep looking until you find someone who can walk that path with you.
POCD can feel isolating, but it is a well-understood and highly treatable form of OCD.
At KDH Counseling, we work with intrusive thoughts and OCD using Exposure and Response Prevention (ERP), a specialized form of cognitive behavioral therapy (CBT). Our clinicians are trained in evidence-based OCD treatment and approach this work with both precision and respect for your experience.
We provide OCD therapy in Lafayette, Louisiana, with in-person and telehealth options available across the state.
If this feels familiar, you don’t have to navigate it alone. You can learn more about our OCD services or schedule a consultation to get started.
POCD flourishes in silence. ERP invites people to speak. To say, “I’m having thoughts I hate. And I’m terrified they mean something. But I want to get better.”
There is no help in secrecy, but there is help in honesty. In the tender, terrifying work of sitting beside your own fear repeatedly. Either you habituate or you get used to the thought (Defusion) and it gets easier. This is not because we reassure ourselves or convince ourselves that the OCD isn't true. We face this inner demon in systematic ways and we are changed by the process.
If this is you-or someone you love-please know this:
You are not your thoughts.
You are not alone.
And you are not beyond help.
OCD may be loud, but with the right kind of help, you can be louder.

Question: What is POCD, and why do the thoughts feel so unbearable?
Short answer: POCD is a subtype of OCD marked by intrusive, unwanted thoughts or images about sexually harming children that clash violently with a person's values. Clinically, these thoughts are ego-dystonic---they do not reflect attraction or desire. They're not fantasies; they're fears. For example, a loving parent might dread changing a diaper because their mind flashes an image they never wanted. The distress comes from terror and moral misalignment, not intent.
Question: How is POCD different from Pedophilic Disorder?
Short answer: POCD is about fear---fear of being dangerous, losing control, or harming a vulnerable population. Pedophilic Disorder involves an enduring sexual attraction to children, often with justification or lack of remorse. People with POCD are typically horrified by their thoughts and seek to avoid harm. Because the stakes are high, accurate diagnosis by a therapist trained in OCD and ERP is crucial; confusing the two is clinically harmful and ethically reckless.
Question: What do obsessions and compulsions look like in POCD, and why don't reassurance or checking help?
Short answer: Common obsessions include questioning whether a glance was inappropriate, replaying a hug while scanning for intent or groinal sensations, or avoiding eye contact out of fear of what the mind might conjure. Compulsions include avoiding children or places where they are, seeking reassurance (from loved ones or the internet), mentally reviewing interactions, checking bodily sensations, and researching pedophilia. These behaviors create brief relief but strengthen the fear cycle, making OCD louder over time. Chasing certainty feeds the disorder; it never delivers lasting peace.
Question: What is ERP, and what does it look like for someone with POCD? Is it safe?
Short answer: ERP (Exposure and Response Prevention) is a structured, ethical treatment that helps you build tolerance to uncertainty and discomfort by facing triggers and preventing compulsions. It does not involve illegal or harmful behavior. Examples include: looking at a photo of a child and allowing the thoughts to come without neutralizing them; writing and repeatedly reading an exposure script with a therapist until it loses its sting; or spending time with nieces/nephews while abstaining from post-event mental review. Repetition teaches the nervous system that distress is survivable, and the thoughts lose their edge. ERP isn't punishment-it's a courageous, guided practice in not letting fear make your choices.
Question: Do I need medication, and how do I find the right ERP therapist?
Short answer: Medication (such as SSRIs) can help some people, but ERP alone is effective for many, with a 70--80% success rate when done properly. When choosing a therapist, look for: specific training in ERP (e.g., BTTI/IOCDF-related training), comfort with taboo intrusive thoughts without reassurance, extensive OCD experience (not just general anxiety work), a grounded, nonjudgmental stance, and a focus on doing exposures rather than analyzing why the thoughts occur. You deserve treatment that honors your bravery and offers a clear path forward.

Some fears arrive like thunderstorms-loud, visible, and unmistakable. Others creep in quietly, like fog-unwelcome, disorienting, and hard to explain....
I began working with individuals who have OCD about 10 to 12 years ago. My journey into understanding OCD started in graduate school, where I was...

Many clients ask me, “What exactly is ERP?” Exposure and Response Prevention Treatment, or ERP, may sound formal or technical, but at its core, it is...