
 KDH Team
KDH Team
What it is Brainspotting and How it Can Help?
Discover how Brainspotting vs EMDR can be used more efficiently to work with trauma. What is Brainspotting? Branspotting (BSP) therapy is a powerful...

A nervous-system healing that starts with how humans process fear.
People often arrive in therapy acutely aware of their current symptoms. They know their trauma history or at least know what happened, but they may not understand why their body still reacts as if the danger is present. They can tell the story clearly. They’ve talked it through without feeling many emotions when they tell their story. And yet anxiety keeps showing up-tight chest, racing thoughts, a sense of urgency that doesn’t match the moment, chronic rumination, and much more.
To understand why EMDR therapy for anxiety can be so effective, we need to zoom out first and talk about something more general: IVR.

IVR (Imaginal Vivid Recall), in therapy, refers to imaginal-based reprocessing, often described as imaginal exposure or imaginal vivid recall. It’s a broad category of therapeutic work where a person intentionally brings an internal experience (a memory, image, feared scenario, or body sensation) into awareness so the nervous system can learn something new about it.
IVR shows up in many evidence-based therapies:
The common thread is this:
the brain revisits an internal representation of fear while remaining physically safe in the present.
Why does this matter? Because the nervous system learns primarily through experience, not logic. Avoidance keeps fear alive. Carefully structured internal exposure gives the brain a chance to update outdated threat responses.
When done well, IVR allows the nervous system to discover:
But IVR alone can be taxing. For some clients, simply imagining feared material keeps the nervous system in a loop of effortful control-white-knuckling through fear rather than metabolizing it.
This is where EMDR becomes something more than traditional IVR.
EMDR stands for Eye Movement Desensitization and Reprocessing. The simplest, most accurate EMDR definition is this:
EMDR therapy is an evidence-based therapy that helps the brain reprocess distressing experiences so they are stored as completed (it's over now), past events rather than ongoing threats.
EMDR is rooted in the Adaptive Information Processing (AIP) model, which proposes that symptoms arise when experiences overwhelm the brain’s natural ability to integrate information. Memories then remain “stuck” with their original sensations, emotions, and beliefs intact.
Unlike traditional IVR, EMDR does not rely on sustained effortful exposure. Instead, it pairs brief, titrated attention to internal material with bilateral stimulation (eye movements, taps, or tones). This combination appears to engage natural memory-processing mechanisms similar to those involved in REM sleep.
The result is not suppression or forced calming. It’s integration.
EMDR was developed by Francine Shapiro, and over the last three decades has been supported by extensive peer-reviewed research across trauma and anxiety-related conditions.

EMDR absolutely includes IVR. Clients still bring internal material into awareness. Memories, images, sensations, beliefs, and emotions are all part of the process.
The difference is how long the system stays there and what happens next.
In EMDR:
Instead of repeatedly confronting fear, the system begins to link the memory to adaptive information-current safety, adult capacity, contextual understanding.
This is why clients often say things like:
That shift is the hallmark of reprocessing rather than endurance.
Anxiety is often misunderstood as a thinking problem. In reality, anxiety is frequently a memory and threat-prediction problem.
The nervous system learned-sometimes early, sometimes repeatedly-that the world is unpredictable, overwhelming, or unsafe. Even when there is no single “big trauma,” anxiety can be rooted in:
EMDR therapy for anxiety targets the memory networks that taught the body to stay on high alert.
Rather than starting with symptom control, EMDR asks:
Through EMDR, anxiety triggers are linked back to earlier experiences and reprocessed so the nervous system no longer treats present-day cues as emergencies.
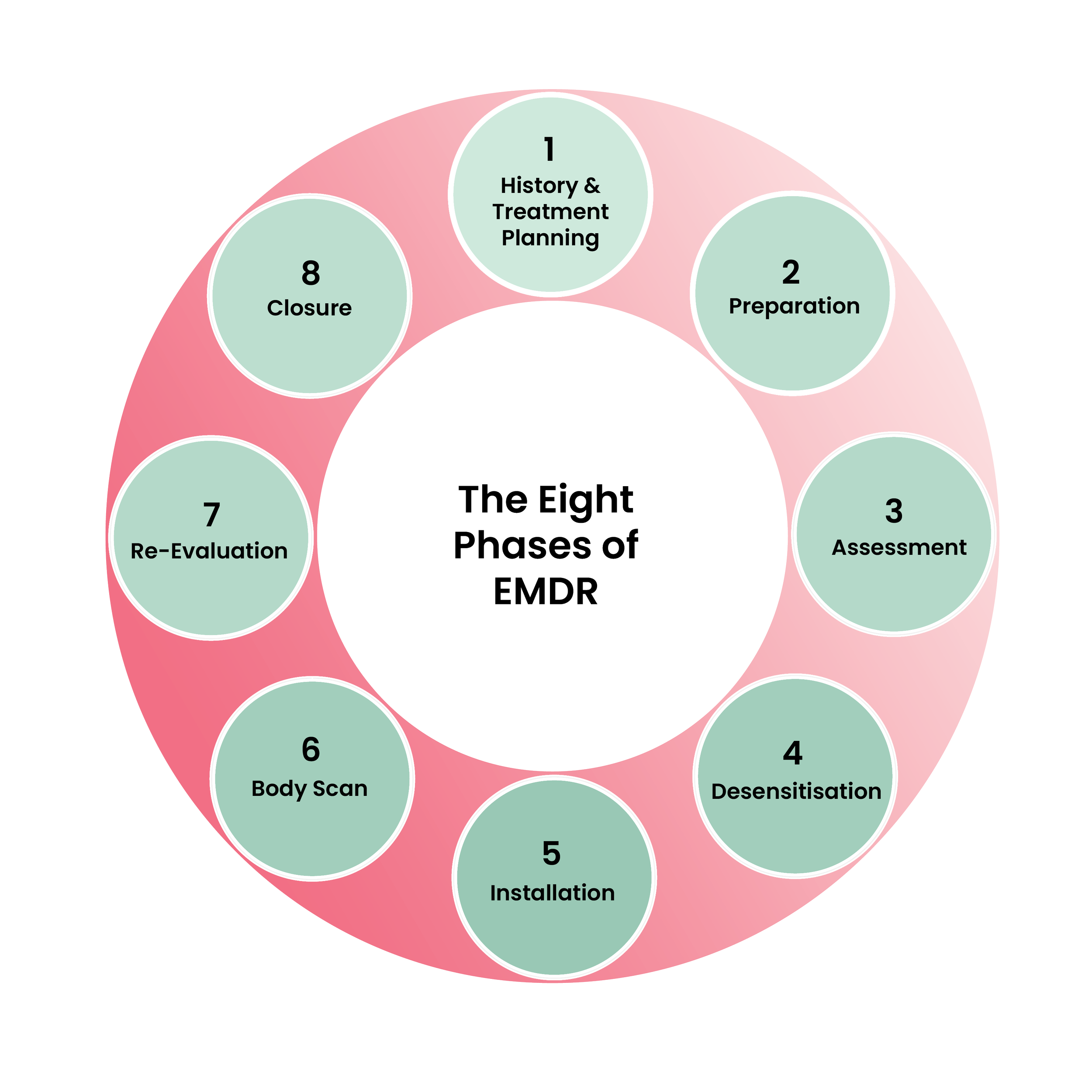
EMDR therapy follows a structured eight-phase protocol, which is especially important when working with anxiety:
Clients do not need to “push through” panic. Sessions are paced. Regulation is prioritized. This makes EMDR particularly effective for people whose anxiety escalates quickly or becomes somatic.
Research suggests EMDR reduces hyperactivation in the amygdala while increasing connectivity with cortical regions responsible for meaning, orientation, and regulation. In practical terms, this means:
Multiple peer-reviewed studies show EMDR to be as effective as CBT for anxiety disorders, with some evidence of faster symptom reduction when anxiety is trauma-linked.
Importantly, EMDR does not require detailed verbal recounting or prolonged exposure-making it more accessible for clients who become overwhelmed by traditional IVR approaches.
EMDR therapy is:
EMDR therapy is not:
Skilled assessment matters. Preparation matters. The relationship matters.

It’s also important to recognize that not every nervous system processes information in the same way. For some neurodivergent clients-particularly individuals with autism, ADHD, sensory processing differences, or a history of strong dissociation-the rapid eye movements used in EMDR can sometimes feel overstimulating or difficult to track.
Research on neurodivergence and trauma increasingly highlights that sensory load, attentional shifts, and rapid visual tracking can create fatigue or disorientation for certain clients. When that happens, the goal isn’t to force the method to work; the goal is to respect how the nervous system processes experience. In these situations, clinicians may consider alternative brain-based trauma therapies that rely less on continuous eye movements.
Approaches such as Deep Brain Reorienting (DBR) or Brainspotting can sometimes be better fits. These methods tend to work more slowly with the orienting response and subcortical processing systems of the brain, allowing clients to stay more present while trauma material unfolds.
The broader lesson is that trauma therapy is not one-size-fits-all. Different nervous systems benefit from different pathways into healing, and thoughtful clinicians adapt the method to the person rather than expecting the person to adapt to the method
At its core, IVR-based therapies remind the nervous system that fear can be approached rather than endlessly avoided. Avoidance keeps the alarm system alive; carefully returning to internal experiences in a safe environment allows the brain to update what it once learned under pressure.
EMDR therapy builds on that same principle by supporting the brain’s natural ability to process experience through bilateral stimulation and structured reprocessing. For many people, including those seeking EMDR therapy, this approach allows distressing memories and fear responses to finally move from a state of constant activation into something the brain recognizes as past.
It’s also important to remember that healing pathways may look different depending on how someone’s nervous system works. Some neurodivergent individuals who experience high levels of dissociation, may find that rapid eye movements are not the most comfortable or effective entry point for trauma work. In those cases, you may explore approaches such as Deep Brain Reorienting (DBR) or Brainspotting, which work more gradually with the brain’s orienting and subcortical systems. These therapies still follow the same core goal-helping the nervous system process what it once could not-but they do so in ways that may feel steadier for certain bodies and minds.
Because mental health symptoms are not a personal failure of coping. It is usually a nervous system that learned something once and has not yet had the chance to update that learning. Therapies like EMDR, DBR, and BSP, create the conditions for that update to happen. Not by forcing calm or pushing someone past their limits, but by allowing the nervous system to finish what it started.
And when the brain finally completes that unfinished processing, the changes holds.


Discover how Brainspotting vs EMDR can be used more efficiently to work with trauma. What is Brainspotting? Branspotting (BSP) therapy is a powerful...

Many people come into therapy looking for relief from their thoughts. They might say, “I just want to stop overthinking,” or “I want the anxiety to...

In a world full of complexities and contradictions, it's not uncommon to feel overwhelmed by emotions or find yourself in constant conflict with...